Trigger Point Therapy for Myofascial Pain (8 page)
Read Trigger Point Therapy for Myofascial Pain Online
Authors: L.M.T. L.Ac. Donna Finando

John Upledger has referred to the fascia as “a single and continuous laminated sheet of connective tissue . . . [which] extends without interruption from the top of the head to the tips of the toes. It contains pockets which allow for the presence of the viscera, the visceral cavities, the muscles and skeletal structures.”
2
The complex, interactive nature and homeodynamic activity of this system must be appreciated and respected.
As practitioners we have come to experience a fundamental state of awe that is with us each day as we treat our patients. The complexity and beauty of the myofascial system has led us to experience some amusement when a patient, learning of the nature of his or her condition, remarks, “You mean it's
just
muscular?” Exactly. It's
just
the Grand Canyon.
CHAPTER 5
H
OW
TO
U
SE
T
HIS
M
ANUAL
T
his manual provides important information in a format that can be easily and quickly accessed by both the student and the working health care practitioner, making it readily useable in the clinic or office.
In the technical body of the book an illustration of each muscle and the locations of its common trigger points is accompanied by the following information:
Proximal attachment:
The cephalad (upper) attachment, that is, the attachment closest to the head.
Distal attachment:
The caudad (lower) attachment, that is, the attachment farthest away from the head.
1
Action:
What the muscle moves, the purpose of its action.
Palpation:
Specific instructions on how to locate and palpate the muscle, including anatomical landmarks for reference.
Pain pattern:
An illustration of that muscle's essential pain pattern is accompanied by a written description that also details possible extended pain patterns. Symptoms produced by the presence of trigger points in the muscle are also described.
Causative or perpetuating factors:
A description of common behaviors that either produce or perpetuate the pain.
Satellite trigger points:
Additional muscles and muscle groups that commonly develop trigger points when there are trigger points in the muscle.
Affected organ systems:
Due to the relationship between skeletal muscle and meridian pathway, the constriction of each muscle or muscle group will affect the meridian pathway traversing it. As each meridian exercises influence over a specific organ or system, this section may shed additional light on the interaction between skeletal muscle and viscera.
Associated zones, meridians, and points:
A statement of other areas predisposed to muscular constriction when there are trigger points in a particular muscle, to guide treatment for those practicing from an Oriental medical perspective. For a review of meridian pathways and zone description, see appendices 1 and 2.
Stretch exercises:
Illustrations and descriptions of stretching exercises useful for that particular muscle. Varying levels of stretch exercises may be provided to patients to accommodate their changing capacities during the healing process.
Strengthening exercises:
A description of useful strengthening exercises for the muscle and associated muscle groups. A strengthening exercise is included for phasic muscles, which tend toward weakening. Tonic, or postural muscles, tend toward shortening, making strengthening exercises generally unnecessary.
Regarding the trigger point illustrations, it must be remembered that they serve only as a means to guide the initial palpation, since trigger points can present at any point in any muscle.
Most patients present with symptoms that are usually described as a particular pattern of pain. Some patients will also present with other symptoms, such as impaired range of motion, usually described as an inability to perform particular tasks. Other symptoms might seem less related, such as dizziness or menstrual problems. Two indexes are provided in an effort to help the practitioner quickly focus his or her attention on muscle groups that commonly relate to the pain pattern or symptoms presented by the patient.
The Pain Pattern Index is a graphic index in which the pain patterns for each muscle are illustrated. The pain patterns are grouped in terms of the area affected: pain patterns that affect the neck are shown together, pain patterns that affect the anterior legs are shown together, and so on. With this information ready comparisons of patterns can be made and specific information about the muscle groups quickly located.
Some patients may be vague about their pain but clear on other symptoms. The Symptom Index provides common symptoms of myofascial syndromes and the page numbers of related muscles.
Using the indexes to help narrow the focus to particular muscles involved, then turning to the summary information for each muscle, should help guide examination, treatment, and follow-up with the patient.
This manual is designed for quick access for use in clinical situations. The material is meant to supplement and guide the careful taking of case history, examination, and palpation, not to replace them.
This manual does not outline each muscle of the body. The muscles that have been included are those that we have found to be the most clinically significant in our years of practice. Pain experienced by the great majority of patients may be alleviated through the treatment of these muscle groups. For an indepth discussion of each muscle in the body, use of
Myofascial Pain and Dysfunction: The Trigger Point Manual
(volumes I and II) by Travell and Simons is recommended.

Â
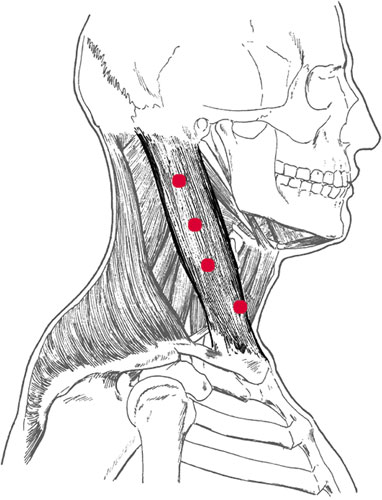
Sternocleidomastoid and trigger points
S
TERNOCLEIDOMASTOID
Proximal attachment:
Mastoid process and the lateral half of the superior nuchal line of the occipital bone.
Distal attachment:
Clavicular head:
superior border of the anterior surface of the medial one-third of the clavicle.
Sternal head:
anterior surface of the manubrium, medial and more superficial than the clavicular head.
Action:
Acting unilaterally:
rotation of the face to the opposite side and lifting the chin; aids in sidebending to the same side.
Acting bilaterally:
flexion of the head and neck; checkreins backward motion of the head during chewing; auxillary muscle of inspiration.
Palpation:
To locate the sternocleidomastoid (SCM), identify the following structures:
- Mastoid processâFollow the base of the occiput toward its lateral edge. The rounded, most lateral prominence is the mastoid process.
- ClavicleâFollow the curved course of the clavicle, from its articulation with the sternum to its articulation with the acromion. Medially the contours of the clavicle are convex; laterally its contours are concave.
- Sternoclavicular articulationâLocate the suprasternal notch at the superior aspect of the manubrium. Move laterally to locate the sternoclavicular articulation. Note that the clavicle is raised slightly above the manubrium at the articulation. By raising and lowering the shoulder as you palpate the articulation, you can clearly distinguish between the manubrium and the clavicle.
- Transverse process of C1âLocate the angle of the mandible, the sharp, lateral aspect of the jawbone. Moving posteriorly, the bony prominence of the transverse process of C1, lying between the angle of the mandible and the mastoid process, may be palpated on some people. Palpate bilaterally, gently, as this area may be quite tender.
To palpate the sternocleidomastoid, begin at the mastoid process with the patient lying supine. Locate the thickened proximal aspect of the SCM. Use your index finger to border the muscle's medial aspect and your ring finger to border its lateral aspect. Place your middle finger along the belly of the muscle and follow it down to the attachments on both the manubrium and the clavicle. Tilt the chin up toward the opposite side to differentiate clearly between the sternal attachmentâthin and cordlike at its insertionâand the broader, flatter clavicular attachment on the upper surface of the clavicle.
It is interesting to note that the SCM and the trapezius have a continuous attachment along the base of the occiput. This attachment splits at the mastoid process. They have a noncontinuous attachment along the superior border of the clavicle.
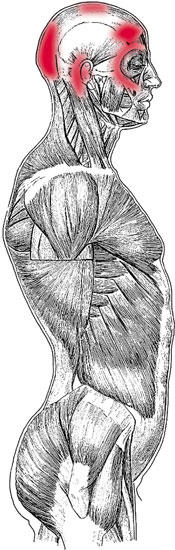
Sternocleidomastoid pain pattern
Pain pattern:
Clavicular head:
Pain refers to the frontal areaâwhen severe, it extends across the forehead to the opposite side. Homolateral pain deep in the ear. Symptoms are frontal headache, dizziness, and postural imbalance.
Sternal head:
Cheek, temple, and orbit pain; pain that arches across the cheek and into the maxilla, over the supraorbital ridge. Vertex pain with scalp tenderness. Symptoms include dry cough and autonomic phenomena of the eye, including tearing and redness.
Causative or perpetuating factors:
Mechanical overload in extension or flexion; chronic rotation to one side; whiplash; compression of the neck; paradoxical breathing or chronic cough.
Satellite trigger points:
Contralateral SCM, scalenes, levator scapulae, trapezius, splenius cervicis, sternalis, pectoralis major.
Affected organ systems:
Respiratory system; eyes, ears, throat; nasal sinuses.
Associated zones, meridians, and points:
Ventral and lateral zones; Foot Yang Ming Stomach meridian; ST 10, 11, and 12; CO 17 and 18; SJ 16; SI 16.
Stretch exercises:
- Clavicular head:
Bend head and neck backward, rotating the face to one side. The muscle will be stretched at the clavicular head on the opposite side. - Sternal head:
Turn head to one side, then at full rotation tilt the chin toward the shoulder. The muscle will be stretched at the sternal head on the same side.
Strengthening exercises:
Isometric against mild forward resistance.
- Place the palm heel on the forehead for resistance. Press the forehead into the resistance.
- Clasp the hands behind the head, just below the crown. Press the head and neck posteriorly, against the resistance.
