Trigger Point Therapy for Myofascial Pain (22 page)
Read Trigger Point Therapy for Myofascial Pain Online
Authors: L.M.T. L.Ac. Donna Finando

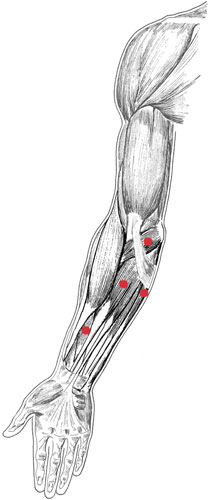
Hand and finger flexors and trigger points
H
AND
AND
F
INGER
F
LEXORS
F
LEXOR CARPI RADIALIS
, P
ALMARIS LONGUS
, F
LEXOR DIGITORUM SUPERFICIALIS
, F
LEXOR CARPI ULNARIS
1
Proximal attachment:
Flexor carpi radialis:
medial epicondyle of the humerus via the common flexor tendon.
Palmaris longus:
medial epicondyle of the humerus via the common flexor tendon.
Flexor digitorum superficialis:
medial epicondyle of the humerus via the common flexor tendon, medial aspect of the coronoid process of the ulna, and proximal one-half of the radius.
Flexor carpi ulnaris:
medial epicondyle of the humerus via the common flexor tendon and proximal two-thirds of the posterior ulna.
Distal attachment:
Flexor carpi radialis:
base of the second and possibly the third metacarpal.
Palmaris longus:
palmar aponeurosis.
Flexor digitorum superficialis:
middle phalange of each of the four fingers.
Flexor carpi ulnaris:
pisiform bone.
Action:
Flexor carpi radialis:
flexion and radial deviation of the hand.
Palmaris longus:
flexion of the hand.
Flexor digitorum superficialis:
flexion of the middle phalange of each of the four fingers.
Flexor carpi ulnaris:
flexion and ulnar deviation of the hand.
Palpation:
Each of the superficial muscles of the ventral forearm can harbor constrictions that may be the source of myofascial pain. Palpate these muscles with the forearm fully supinated and the hand and fingers extended. Locate areas of constriction using digital palpation along the ventral (anterior) forearm, following the course of each muscle as it moves from its proximal position on the forearm to the wrist and hand. In order to identify each muscle, move the hand and fingers through the actions performed by each individual muscle as you palpate. While flexor carpi radialis, palmaris longus, and flexor carpi ulnaris may be palpated throughout their course, flexor digitorum superficialis may be palpated in the distal one-third of the forearm, in between the tendons of brachioradialis and flexor carpi radialis on the radial side and between the tendons of palmaris longus and flexor carpi ulnaris on the ulnar side.

Hand and finger flexors pain pattern
Pain pattern:
Finger pain; possibly a “trigger finger,” in which the interphalangeal joint locks in flexion; pain with repetitive forceful or extensive flexion of the hand and fingers;
Palmaris longus:
pain radiating into the center of the palm of the hand.
Causative or perpetuating factors:
Repetitive or prolonged gripping, twisting, or pulling movements of the hand and fingers.
Satellite trigger points:
Each of the hand and finger flexors may develop satellite trigger points in response to the presence of trigger points in any other muscle of the group.
Affected organ systems:
Respiratory and cardiovascular systems.
Associated zones, meridians, and points:
Ventral zone; Hand Tai Yin Lung meridian, Hand Jue Yin Pericardium meridian, Hand Shao Yin Heart meridian; LU 5â9, HE 3â7, PC 3â7.
Stretch exercise:
Slowly press the fingers and wrist into extension using the opposite hand or by pressing the palm and fingers down onto a flat surface while keeping the elbow straight. Hold for a count of five to ten.
Strengthening exercise:
Form a light fist while maintaining a neutral or slightly extended wrist position. With the elbow fully extended, flex the wrist. Return to a neutral position.
Repeat eight to ten times. Light hand weights may be used to increase the work effort of the hand flexors.
Stretch exercise: Hand and finger flexors
Â
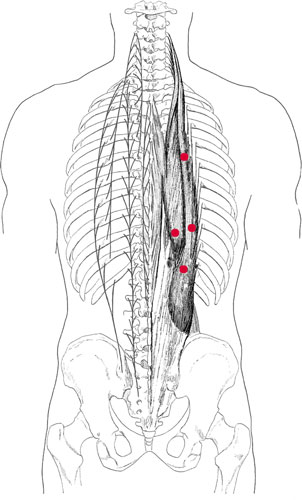
Erector spinae and trigger points
E
RECTOR
S
PINAE
I
LIOCOSTALIS
T
HORACIS
, I
LIOCOSTALIS
L
UMBORUM,
L
ONGISSIMUS
T
HORACIS,
S
PINALIS
Of the three muscles identified as part the erector spinae group (iliocostalis, longissimus, and spinalis), iliocostalis and longissimus are considered to be the most clinically significant in most cases. The spinalis is the most medially placed muscle of the group. It is generally poorly developed and has little clinical significance; it is therefore not included in our discussion.
Proximal attachment:
Iliocostalis thoracis:
angles of the upper six ribs.
Iliocostalis lumborum:
angles of the lowest six ribs.
Longissimus thoracis:
transverse processes of all thoracic vertebrae and adjacent ribs.
Distal attachment:
Iliocostalis thoracis:
angles of the lowest six or seven ribs.
Iliocostalis lumborum
and
longissimus thoracis:
via the shared lumbocostal aponeurosis of the erector spinae, attaching to the transverse processes of the lumbar vertebrae (L1âL5) and to the sacrum, iliac crest, and spinous processes of the lumbar vertebrae.
Action:
Acting bilaterally:
extension of the trunk.
Acting unilaterally:
lateral bending to the same side. The erector spinae muscles contract strongly while coughing or straining to have a bowel movement.
Palpation:
The erector spinae are the superficial layer of the paraspinal muscles. They are considered the “true” back muscles due to their work of maintaining posture and their direct action on movement of the vertebral column.
For the purpose of palpation, iliocostalis and longissimus should be considered as one group. To locate iliocostalis and longissimus, identify the following structures:
- Spinous processes of T1âT12
- Spinous processes of L1âL5. Note the change in shape and size of the lumbar spinous processes as compared to the thoracic spinous processes.
- Sacrum
- Iliac crestâLying on a horizontal line with the junction of L4âL5
To palpate the erector spinae, place your hands parallel to the spine, fingers together, hands flat and relaxed, with your index fingers adjacent to but not touching the spinous processes. With firm but gentle pressure, palpate through the overlying trapezius and latissimus dorsi. Your hand movement follows the vertical course of fiber direction. As you move throughout the course of the muscle you may note cord- or ropelike consistency within areas of the musculature. This is a commonly found indicator of myofascial constriction.
You may begin at either end of the spine, but palpate bilaterally and throughout the course of the musculature to assess the condition of the complete muscle group. Differentiate between the superficial musculature and the deeper erector spinae by noting the direction of the muscle fibers. Note that it may be difficult to differentiate between iliocostalis and longissimus.
Focus on the palpation of iliocostalis thoracis by assessing the condition of the most laterally placed vertical bands of muscle lying lateral to T1âT12. Focus on the palpation of iliocostalis lumborum by assessing the condition of the most laterally placed vertical bands of muscle lying lateral to T7âT12 and extending downward over the lumbar region to the sacrum and iliac crests.
To palpate longissimus thoracis, begin close to the transverse processes of the thoracic vertebrae and the adjacent ribs. Follow fiber direction to the lumbar region where the lumbocostal aponeurosis attaches to the sacrum and iliac crests. With focused palpation, try to differentiate between the laterally placed slips of iliocostalis and the more medially placed slips of longissimus. It may be difficult to differentiate the two groups.
Pain pattern:
Iliocostalis thoracis:
pain in the thoracic region of the back and sometimes the abdomen, with restriction of spinal motion.
Iliocostalis lumborum:
pain is referred downward, low in the buttock and along the iliac crest.
Longissimus thoracis:
pain is referred low in the buttock. When trigger points are located bilaterally at the level of L1, the patient will have difficulty rising from a chair and/or climbing stairs.
Causative or perpetuating factors:
Sudden overload through improper lifting; sustained overload resultant from postural stresses (hyperlordosis); immobility for extended periods of time.
Satellite trigger points:
Each muscle of the erector spinae group may develop satellite trigger points in response to the presence of trigger points in any other muscle of the group. Additional trigger points might also be found in the latissimus dorsi and quadratus lumborum muscles.
Affected organ systems:
Due to the placement of the
shu
(chronic disease) points along this region, constriction of regions of this muscle may reflect the condition of the following organs.
Iliocostalis thoracis:
lung, stomach, gallbladder, liver, and spleen.
Iliocostalis lumborum:
stomach, gallbladder, liver, spleen, kidney, and colon.
Longissimus thoracis:
lung, stomach, gallbladder, liver, spleen, kidney, and colon. We have observed constriction in this muscle between T6 and T12 in patients suffering with diabetes.