Trigger Point Therapy for Myofascial Pain (15 page)
Read Trigger Point Therapy for Myofascial Pain Online
Authors: L.M.T. L.Ac. Donna Finando

Ask the patient to lie supine with his forearm resting comfortably on his body at the level of his waist. Ask him to bring his shoulder forward (anterior) by lifting his scapula off the table and then to take a deep breath. Palpation at the area of pectoralis minor will note the then-activated muscle. Palpate through pectoralis major to detect constricted fibers of pectoralis minor.
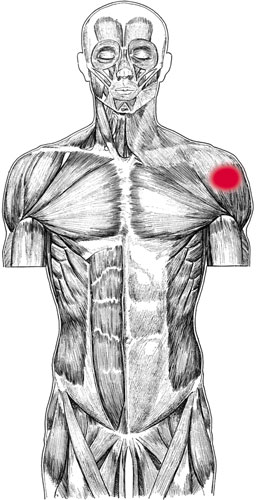
Pectoralis minor pain pattern
Pain pattern:
Pain is referred to the front of the shoulder (anterior deltoid region) and possibly the front of the chest; some pain may be referred down the ulnar aspect of the arm to the fourth and fifth digits. Symptoms may include limitation in reaching forward and up or in reaching backward with the arm at the level of the shoulder.
Causative or perpetuating factors:
Stooped, forward-leaning posture; compression, as that which might occur from the pressure of a backpack strap on the area.
Satellite trigger points:
Pectoralis major, anterior deltoid, scalenes, sternocleidomastoid.
Affected organ system:
Respiratory system.
Associated zones, meridians, and points:
Ventral zone; Hand Tai Yin Lung meridian; SP 19 and 20.
Stretch exercise:
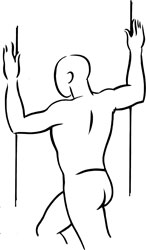
With the forearms placed firmly on each side of a doorway, the palms approximately at ear level, stretch the body through the outstretched arms, opening the chest and anterior shoulder region. It is essential that the stretch is sufficient to retract the scapulae.
Strengthening exercise:
Because the pectoralis minor is a postural muscle, strengthening exercises are generally not necessary.

Stretch exercise: Pectoralis minor
Â
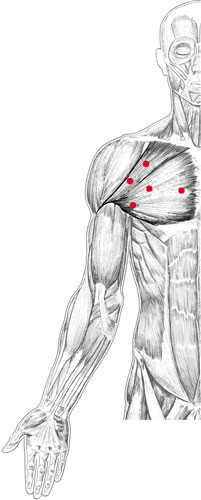
Pectoralis major and trigger points
P
ECTORALIS
M
AJOR
Proximal attachment:
Medial two-thirds of the clavicle; sternum; costal cartilages of ribs 2â7; superficial aponeuroses of the external oblique and rectus abdominis.
Distal attachment:
Lateral lip of the bicipital groove of the humerus.
Action:
Adduction and medial rotation of the arm.
Clavicular fibers:
flexion of the arm, as in touching the lobe of the opposite ear.
Palpation:
Pectoralis major forms the anterior wall of the axilla. As a superficial muscle of the chest wall, pectoralis major is clearly observable when the patient presses medially against his iliac crest.
To locate pectoralis major, identify the following structures:
- ClavicleâFollow the curved course of the clavicle, from its articulation with the sternum to its articulation with the acromion. Medially the contours of the clavicle are convex; laterally its contours are concave.
- SternumâThe breastbone: a long, flat bone that forms the center of the anterior thorax.
- Bicipital groove of the humerus (intertubercular groove)âIdentify the greater and lesser tuberosities of the humerus, just distal to the lateral aspect of the acromion. (These are best palpated with the arm externally rotated.) The bicipital groove lies medial to the greater tuberosity and lateral to the lesser tuberosity. Note that the tendon of the long head of the biceps brachii runs through the bicipital groove.
Locate pectoralis major with the patient lying supine, his arm resting at his side. Palpate pectoralis major throughout its course, beginning at its medial attachment at the sternum and the medial two-thirds of the distal aspect of the clavicle. Move laterally across the chest wall to its lateral attachment at the bicipital groove. The lateral aspect of the muscle, its free edge, may be lifted slightly off the chest wall in order to directly palpate the fibers using a pincer grasp palpation technique.
Pain pattern:
Pain in the anterior aspect of the shoulder, at the anterior deltoid region; the pain pattern may include the anterior chest and breast. Pain may extend down the ulnar aspect of the arm to the fourth and fifth digits. Pain may sometimes mimic angina pectoris.
Causative or perpetuating factors:
Overload stresses due to heavy lifting with arms in front of the body; immobilization of the arm in an adducted position; sustained round-shouldered position; sustained anxiety levels; referred phenomena via a viscerosomatic route associated with cardiac infarction.
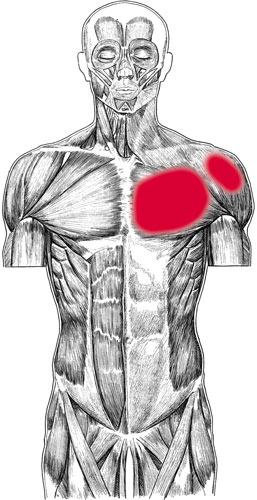
Pectoralis major pain pattern
Strengthening exercise:
Lie in the supine position, arms abducted to 90 degrees and palms facing the ceiling. Horizontally flex the arms across the chest, keeping the elbows straight. Slowly return the arms to the starting position. Repeat five to ten times, flexing to a count of two and returning to the starting position to a count of four.
Satellite trigger points:
Anterior deltoid, sternocleidomastoid, scalenes, trapezius, rhomboids.
Affected organ systems:
Respiratory and cardiovascular systems.
Associated zones, meridians, and points:
Ventral zone; Foot Yang Ming Stomach meridian, Hand Tai Yin Lung meridian, Foot Tai Yin Spleen meridian, Foot Shao Yin Kidney meridian; ST 14, 15, and 16; ST 18; LU 1, 2, and 3; SP 19 and 20; KI 22â27.
Stretch exercise:
With the forearms placed firmly on each side of a doorway, stretch the body through the outstretched arms, opening the chest and anterior shoulder region.
1.   Place the palms approximately at ear level to stretch the upper fibers of pectoralis major.
2.   Place the elbows level with the shoulders to stretch the middle fibers of pectoralis major.
3.   Extend the arms fully, placing the hands well above the level of the head to stretch the lower fibers of pectoralis major.
Stretch exercise 1: Pectoralis major

Stretch exercise 2: Pectoralis major

Stretch exercise 3: Pectoralis major

Deltoid (anterior) and trigger points