Read Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine Online
Authors: Marc Sabatine
Tags: #Medical, #Internal Medicine
Pocket Medicine: The Massachusetts General Hospital Handbook of Internal Medicine (76 page)

• Most common cause of cancer-related death for both men and women in the U.S.
•
Cigarette smoking
: 85% of lung cancers occur in smokers; risk ∝ total pack-yrs, ↓ risk after quitting/reducing, but not to baseline (
Int J Cancer
2012;131:1210) squamous & small cell almost exclusively in smokers adenocarcinoma most common type in nonsmokers bronchioalveolar carcinoma associated with women, nonsmokers,
EGFR
mutations • Asbestos: when combined with smoking, synergistic ↑ in risk of lung cancer • Radon: risk to general population unclear
Clinical manifestations
• ~10% are asx at presentation and are detected incidentally by imaging •
Endobronchial growth
of 1° tumor:
cough
,
hemoptysis
,
dyspnea
, wheezing, post– obstructive pneumonia; more common with squamous or small cell (central location) •
Regional spread
pleural effusion
, pericardial effusion, hoarseness (recurrent laryngeal nerve palsy), dysphagia (esophageal compression), stridor (tracheal obstruction)
Pancoast’s syndrome
: apical tumor → brachial plexus involvement (C8, T1, T2) → Horner’s syndrome, shoulder pain, rib destruction, atrophy of hand muscles
SVC syndrome
(
NEJM
2007;356:1862): central tumor → SVC compression → face or arm swelling (>80%), venous distention of neck & chest wall (~60%), dyspnea/cough (~50%), HA (~10%); Rx = steroids & diuretics, RT ± chemo after tissue dx, SVC stent for severe sx, fibrinolytic + anticoag if thrombus
•
Extrathoracic metastases
: brain, bone, liver, adrenal •
Paraneoplastic syndromes
Endocrine
:
ACTH (SCLC) →
Cushing’s syndrome
; ADH (SCLC) →
SIADH
PTH-rP (squamous cell) →
hypercalcemia
Skeletal
: digital clubbing (non–small cell),
hypertrophic pulmonary osteoarthropathy
(adenocarcinoma) = symmetric polyarthritis and proliferative periostitis of long bones
Neurologic
(SCLC):
Eaton-Lambert
, peripheral neuropathy, cerebellar degeneration, limbic encephalitis
Cutaneous
: acanthosis nigricans, dermatomyositis
Hematologic
: hypercoagulable state (adenocarcinoma), DIC, marantic endocarditis
Screening
(
JAMA
2011;306:1865;
NEJM
2011;365:395)
• No benefit to CXR or sputum cytology, even in high-risk Pts • Low-dose chest CT in >30 pack-y smokers age 55–74 y → 20% ↓ in lung cancer–related mortality vs. CXR; number needed to screen = 320; high false rate
rate
Diagnostic and staging evaluation
(
NCCN Guidelines
v.3.2012)
•
Initial imaging
: chest CT (include liver and adrenal glands) w/ contrast if possible •
Tissue
bronchoscopy
(for central lesions) or
CT-guided needle bx
(for peripheral lesions or accessible sites of suspected metastasis)
mediastinoscopy (lymph node bx), VATS (eval. of pleura peripheral lesions), thoracentesis (cell block for cytology) or sputum cytology (for central lesions)
•
Staging
Intrathoracic
:
mediastinoscopy
(± preceded by U/S-guided transesoph. or transbronch. needle aspiration;
JAMA
2010;304:2245) or
VATS
; thoracentesis if pleural effusion
Extrathoracic
:
PET-CT
more Se than CT alone for detecting mediastinal and distant mets as well as bone mets (
NEJM
2009;361:32);
brain MRI
for all Pts (except IA)
•
Genetic testing
for
EGFR
mutations and
ALK
rearrang. for stage IV nonsquam NSCLC
• PFTs w/ quantitative V/Q if planned treatment includes surgical resection; need to have 30% of normal, predicted lung fxn
after
resection

NSCLC treatment
(
NCCN Guidelines
v.3.2012)
•
Stages I & II
:
surgical resection + adjuvant chemo
(surgery alone for stage IA) (
NEJM
2004;350:351 & 2005;352:2589) •
Stage III
:
chemoradiation
is main treatment modality
IIIA viewed as potentially resectable (
Lancet
2009;374:379) and IIIB as unresectable neoadjuvant chemoradiation may convert unresectable → resectable
•
Stage IV
:
chemotherapy
↑ survival vs. best supportive care
backbone of therapy is platinum-based doublet; cisplatin/pemetrexed better for adenocarcinoma; cisplatin/gemcitabine better for squamous (
JCO
2008;26:3543)
bevacizumab (anti-VEGF mAb) + chemo ↑ median survival by 2 mo; ↑ risk of bleeding, ∴ do not use if untreated or hemorrhagic brain mets (
JCO
2009;27:5255) or squamous cell (hemoptysis) (
NEJM
2006;355:2542)
if EGFR mutation (a/w improved prognosis): EGFR tyrosine kinase inhibitor (TKI, eg, erlotinib) first-line Rx (
Lancet
2008;372:1809;
NEJM
2010;362:2380 & 2011;364:947)
if ALK rearrangement: ALK TKI (eg, crizotinib) first-line Rx (
Lancet Oncol
2011;12:1004)
TKI toxicities: rash & diarrhea (common); lung & liver injury (rare but potentially serious) palliative radiation used to control local sx caused by tumor or metastasis solitary brain metastasis: surgical resection + brain radiation may ↑ survival

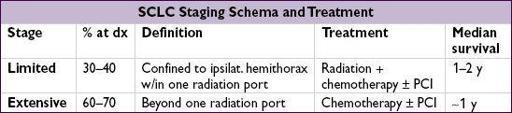
SCLC treatment
(
NCCN Guidelines
v.2.2013)
• SCLC usually disseminated at presentation, but can be very responsive to chemoradiation •
Chemotherapy
(platinum + etoposide) is primary treatment modality •
Thoracic radiation
added to chemotherapy improves survival in limited stage disease •
Prophylactic cranial irradiation
(PCI) improves survival for limited stage disease in complete remission (
NEJM
1999;341:476)
BREAST CANCER
Epidemiology and genetics
(risk assessment tool:
www.cancer.gov/bcrisktool/
)
• In U.S., most common cancer in women; 2nd leading cause of cancer death in women • Age: incidence rates ↑ with age, with possible ↓ in slope after menopause •
Genetics
(
Nature
2012;490:61): Mutations in
TP53
,
PIK3CA
and
GATA3
;
HER2
amplified. 15–20% haveFHx → 2× ↑ risk; ~45% of familial cases a/w known germline mutation
BRCA1/2
: 35–85% lifetime risk of breast cancer & ↑ risk of
ovarian cancer
; ? ↑ colon & prostate cancer; prog not worse than in noncarriers w/ breast ca (
NEJM
2007;357:115); BRCA2: a/w ↑
male
breast cancer & pancreatic cancer. Rare mutations in
CHEK2
,
HRAS
,
TP53
a/w ↑ risk in familial breast cancer (
Breast Cancer Treat Res
2011;127:309)
•
Estrogen
: ↑ risk with early menarche, late menopause, late parity or nulliparity (
NEJM
2006;354:270); ↑ risk with prolonged HRT (RR = 1.24 after 5.6 y,
JAMA
2003;289:3243);
no
↑ risk shown with OCP use (
NEJM
2002;346:2025)
• Benign breast conditions: ↑ risk w/ atypia (atypical ductal or lobular hyperplasia) & proliferative (ductal hyperplasia, papilloma, radial scar or sclerosing adenosis) features;
no
↑ risk w/ cysts, fibroadenoma or columnar changes (
NEJM
2005;352:229) • ↑ risk with h/o ionizing radiation to chest for treatment of Hodgkin lymphoma
Clinical manifestations