Pediatric Primary Care Case Studies (89 page)
Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics

Educate Sam’s mother on the signs and symptoms of clinical deterioration.
When do you want to see this patient back again?

Follow-up for AOM depends on the patient’s age and history of underlying medical problems, particularly speech delay, hearing loss, or learning problems (AAP, 2004). Persistent middle ear effusion after resolution of AOM is typical and should not be seen as treatment failure or need for continued antibiotics. Seventy percent of children will have middle ear fluid at 2 weeks, 40% at 4 weeks, and 10–25% at 3 months (AAP, 2004). Current guidelines recommend follow-up ear checks for all children younger than 2 years. This is typically done at 6 to 8 weeks. It is also recommended that children over 2 years who have a history of speech or developmental delay also be seen for follow-up after AOM (AAP).
Sam’s mother seems to understand the treatment regimen as explained and asks very appropriate questions. When she brings Sam back in 2 months for his previously scheduled 18-month well child visit, he seems to be doing well. On follow-up examination, the right ear is translucent and without erythema, but there is evidence of an air fluid level behind the TM. Pneumatic otoscopy reveals no movement of the TM when positive pressure is applied with the bulb. His left ear is completely normal, as is the remainder of his exam. Sam’s mother reveals that he is doing well developmentally and has a vocabulary of 10 words. Sam’s mother has no concerns with his hearing or speech.
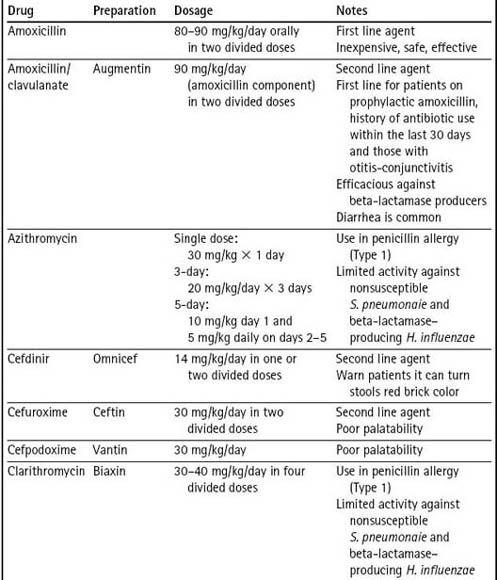
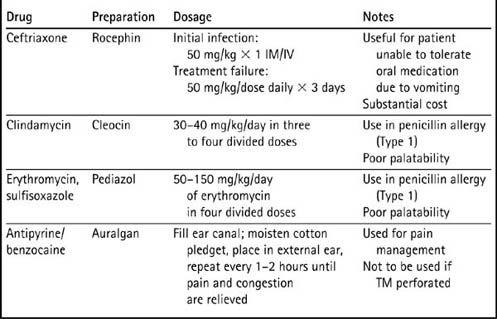
Table 22–2 Agents Used in the Treatment of Acute Otitis Media
Otitis Media with Effusion
Otitis media with effusion, or serous otitis, is present in nearly all children after successful treatment of acute otitis media (Pickering, Baker, Long, & McMillan, 2006). In the majority of patients, OME resolves without medical intervention, but it may take weeks to months to do so. Prolonged OME increases the risk for language delay due to the associated conductive hearing loss. Current guidelines for the management of OME recommend watchful waiting if the patient has no underlying language delays or hearing loss. Hearing tests are recommended if OME persists longer than 3 months, or sooner if language delay, learning difficulties, or hearing loss are suspected. There is no evidence to support the use of antihistamines, decongestants, corticosteroids, or antibiotics in the treatment regimen of OME (American Academy of Family Physicians [AAFP] et al., 2004). Otolaryngology referral is indicated for patients with high risk of speech or learning problems, particularly children with permanent hearing loss, children with craniofacial anomalies or syndromes that affect hearing and eustachian tube function, children with uncorrectable vision loss, and those children with a cleft palate (AAFP et al., 2004).