Murder and Mayhem (4 page)
Authors: D P Lyle

A GSW to the abdomen might be well tolerated by your hero even if it doesn't simply embed in the flesh or muscles of the
abdominal wall (which frequently happens) and actually penetrates the abdominal cavity. It would be very painful, more so than a GSW almost anywhere else, because the internal abdominal lining (peritoneum) is loaded with nerve fibers. But if no major blood vessel or organ (liver, kidney, or spleen) is damaged, your protagonist, if he is tough, could fight through the pain and overcome the enemy. Think James Bond.
A GSW to an extremity seems best for your scenario. This would slow down your hero, but again, unless a major blood vessel was breached, it would not kill or greatly maim him. Besides, the injury could be tailored to hamper your hero's efforts to the greatest degree. If he must chase down the villain, then shoot him in the leg or hip or foot. If he must climb a rope or ladder or wrestle with the antagonist, shoot him in the arm. If he must swim, have the bullet enter his shoulder.
I should also point out that people who suffer severe and potentially lethal GSWs often live long enough to kill their attacker or crawl to a phone or scrawl the killer's name in their own blood. If your protagonist is shot during the climax of your story, the wound could be more serious because he could survive long enough to do in the villain, call for medical help, and heal before the sequel.
Can a Person with Broken Ribs Swim?
Q: One of my characters is hit in the chest while standing on a sailboat and is knocked overboard. I later say that the blow broke a couple of ribs and one of the ribs punctured a lung, causing it to collapse. Using one arm he manages to keep himself afloat for the three or four minutes it takes for someone to haul him back aboard, using the boat's emergency sling.
Would a person with a broken rib, let alone a col-
lapsed lung, be able to use his arm well enough to keep himself afloat? And assuming that this character received competent medical treatment in a modern hospital within two hours of the accident, how long would it be before he could plausibly make his next appearance in the story?
A: A rib fracture is extremely painful, especially since we can't "rest" it or immobilize it while it heals. A broken arm is splinted or placed in a cast; the chest cannot be restricted in this fashion, since breathing is not optional.
Inhaling air into the lungs is an active process. The muscles between the ribs work to expand the chest, creating the negative pressure within the chest cavity required to pull air into the lungs. A fractured rib makes this an extremely painful process.
The pain is typically localized to the area of the fracture and is very sharp—like a knife sticking into the chest. Each breath is excruciating. We call this type of pain "pleuritic." It results not only from the broken rib itself but also from the highly enervated (has a lot of nerves) lining of the chest cavity, called the "pleura."
If the sharp end of the broken rib protrudes into the chest cavity, it may puncture the lung, causing it to collapse. We call this a "pneumothorax." The pneumo (for short) may be small or large, meaning the degree of lung collapse may be minor or significant. We grade these by percentage of collapse. A minor pneumothorax would be 10 to 20 percent, while a large pneumo would be 50 percent or more. A complete collapse would of course be a 100 percent pneumo.
A minor collapse is painful but otherwise not severely debilitating. A complete collapse is painful and associated with marked shortness of breath. It would be lethal only if the victim has significant underlying heart or lung disease or if the pneumo is of the "tension" type. In a tension pneumothorax the hole in the lung acts as a ball valve, or one-way leak (Figure 3a). When the victim inhales, air passes from the lung, through the hole, and into the
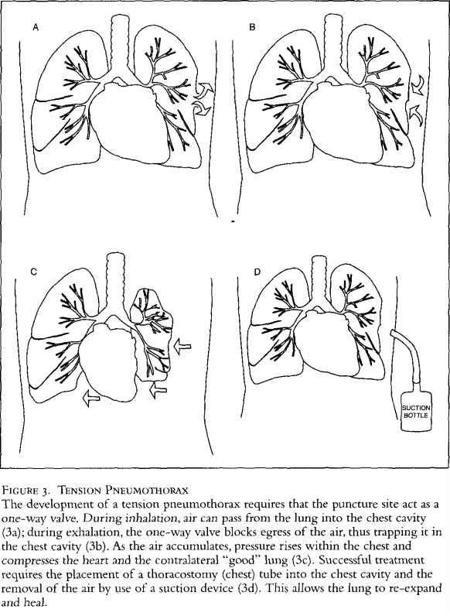
chest cavity (Figure 3a), yet when he attempts to exhale, the air cannot pass back through the hole, into the lung, and out through the mouth (Figure 3b). Each breath increases pressure within the chest, collapsing the lung further. As the pressure (tension) mounts, the heart and the "good" lung also become compressed, resulting in declining heart and lung function and ultimately death (Figure
3c). This may occur rapidly, over minutes. Fortunately, most pneu-mos are not of the tension variety.
Long-term treatment also depends on the degree of collapse. With minor pneumos, the victim is often observed in the hospital for a few days. The leak usually seals itself, the lung reinflates, and the person goes home and experiences a few weeks of chest pain as the fracture heals. When it is a major collapse, a thoracostomy tube (or chest tube) is inserted (Figure 3d). This plastic tube goes through the chest wall and into the chest cavity between the chest wall and the lung. Suction is applied for several days, allowing the lung to reinflate and the leak to heal. The tube is then removed. Subsequent recovery is the same as with a minor leak but may take a couple of weeks longer.
In your scenario a fracture with a minor pneumo would work. Yes, he could swim. Yes, he could fight if necessary. Yes, it would be
very painful, but heroes are forged from pain and perseverance. He could return to action in a few days if absolutely necessary or if he is stubborn and not one to follow doctor's orders.
What Is the Mechanism of Death in a Suicide by Hanging?
Q: A man in my novel commits suicide by tying a rope around his neck and kicking a step stool away. He's dis- covered about half an hour later. Is the cause of death, then, strangulation? Would he have urinated or defecated in the course of dying? Would there be a smell? Also, what would his face look like? Would he have died differently if there was a drop of six feet? Can I assume a different cause of death? Broken neck? Would his face look different? Would his neck be distorted in any way?
A: The result of a hanging depends on several factors—the weight of the victim, the size and muscularity of his neck, and the
distance of the drop, to name a few. If the victim drops several feet, the noose would indeed fracture his neck, and death would be fairly instantaneous. He would simply fall and then hang limply. Yes, he would likely evacuate his bladder and bowels, and the smell would be as expected.
On the other hand, if the fall is short, as in kicking a chair or stool out of the way or having a horse spooked from beneath him—a staple in old Westerns—his neck would not break, and death would be from strangulation. It would be slow and painful, with a great deal of kicking and struggling. When death finally occurs, the victim would likely soil himself as above.
In the latter case, his face would be purplish and engorged with blood. His eyes would protrude; perhaps his tongue would be swollen and protruding; and his neck would be excoriated from the struggle against the rope. Also, the conjunctivae—the pink part of the inside of the eyelid—would show petechial hemorrhages. These look like small bright red spots, and they result from the increased pressure in the veins and capillaries in the tender tissues. Similar findings are common in manual or ligature strangulations.
Most suicides by hanging are poorly executed and the victim does not fracture his neck and thus dies from asphyxiation or strangulation. When the chair is gone and the person finds that he isn't dead, religion and panic take over in short order, and a life-and-death struggle ensues, regardless of how committed the person was to the suicide in the first place. Suddenly, what looked good on paper isn't so attractive. And since in self-hangings the victim usually cannot tie his hands behind his back, he will use them in his struggles for survival. He will claw at his neck or try to climb the rope to ease the pressure of the noose. This results in scratches and tears of the flesh, ripping loose of fingernails, and rope burns on palms and fingers.
What Wounds Would Result from an Attempted Suicide with a Gun Placed Under the Chin?
Q: If a character commits suicide by firing a handgun placed under his chin, and the gun is loaded with "hot loads" (overpowered magnum rounds intended for use against vehicles and similar targets), what kind of ballistic results could be expected? Would the resulting injury produce a relatively small hole due to overpene-tration, or would the mushrooming effect obliterate most of the skull; in other words, is there sufficient resistance to the bullet to cause it to mushroom? Is there a chance of survival, or is this technique highly effective? Aside from "gray matter," is there likely to be much blood?
A: Yes, this is effective and virtually 100 percent fatal provided the gun doesn't slip and the angle change. I saw a man years ago who placed a shotgun under his chin and pulled the trigger. He had angled the barrel slightly forward and opened his face as if someone had cleaved it with an axe. The shot never entered the skull and he was neurologically intact and awake when the paramedics arrived. A plastic surgeon and a neurosurgeon put him back together. But short of such an odd occurrence, this type of approach is uniformly fatal.
Typically, the entry wound is relatively small and the exit wound large, likely removing the entire skullcap and most of the brain. There would be a great deal of tissue and blood. However, a bullet coated with Teflon or otherwise manufactured to "penetrate armor" probably would not "mushroom," and therefore both entry and exit wounds would be small and there would be less tissue and blood. Still effective, but less messy.
Can a Traumatic Miscarriage Prevent Future Pregnancies?
Q: I have a character who is three months pregnant. She is injured in an automobile accident and suffers a miscarriage. Later the doctor tells her she can never have children again. Is this possible? What would have to happen to her to make future pregnancies impossible?
A: Yes, your scenario is possible.
First, let's deal with the accident and the miscarriage. Blunt trauma to the abdomen as occurs in auto accidents (AA) can result in miscarriage. In AAs the seat belt itself can injure the lower abdomen and thus the uterus. If no seat belt is worn, collisions with the steering wheel, dashboard, or seat back (if she is sitting in the backseat) can result in similar injuries. Falls down stairs (a Hollywood staple for this scenario) and kicks or punches, as can occur in domestic abuse situations, can lead to similar injuries.
During pregnancy the fetus floats inside the uterus in amniotic fluid, which serves as some protection from trauma. But if enough force is applied, the fetus can be injured or killed. Or the placenta that nourishes the fetus and is attached to the inner wall of the uterus can be torn loose. Bleeding into the uterine cavity or loss of placental support for the fetus can result in fetal death and miscarriage. In severe trauma the uterus can rupture, and the fetus and even the mother can be lost. As the uterus expands during pregnancy, its walls thin, and it becomes increasingly prone to this catastrophe with each passing month.
If the uterus is intact but the fetus is no longer viable, a dilatation and curettage (D and C) must be done to remove the dead fetus and placenta. Dilatation means the dilating or opening up of the cervix, which the surgeon must do to reach the inside of the
uterus. Curettage is the removal of material from the walls of a cavity—in this case the fetus and placenta from the uterus. If the uterus ruptures, a true medical emergency exists, and surgery must be performed immediately to save the mother. Often the uterus must be removed under these circumstances, though at times it can be repaired and salvaged.
To make future pregnancy impossible, either the uterus itself or its delicate lining would have to be damaged to the point that implantation (the attachment of the fertilized egg to the uterine lining) can no longer occur. Or the uterus could be scarred in such a manner that even if implantation does occur, the uterus cannot support fetal growth and development. After trauma and a D and C, either of these is a possible outcome. Obviously, if the uterus is removed (hysterectomy), pregnancy is precluded.
If your character suffers a uterine rupture in the AA, she would have severe lower abdominal pain and vaginal bleeding, and it is likely she would go into shock: She would be pale, cold, sweaty, delirious, or unconscious, and have a very weak pulse and low blood pressure. The paramedics would begin IVs, give lots of fluids such as D5LR (5 percent dextrose in lactated Ringer's solution), administer oxygen, and speed to the nearest hospital or trauma unit. She would be taken to surgery almost immediately for an emergency hysterectomy. Recovery, if all went well, would take five to seven days in the hospital and then six to eight weeks at home. Of course, the tremendous psychological stress this would cause might take years to overcome.