Welcome to Your Child's Brain: How the Mind Grows From Conception to College (18 page)
Read Welcome to Your Child's Brain: How the Mind Grows From Conception to College Online
Authors: Sandra Aamodt,Sam Wang
Tags: #Pediatrics, #Science, #Medical, #General, #Child Development, #Family & Relationships

For millennia, children could reliably expect to have certain experiences. Infants would hear their parents and other adults talking. Babies would see objects, some of them colored, some of them moving. Food would be obtained from nearby land. The sun would bring light when it rose and leave darkness behind when it set. Our brains evolved to make the most of these situations.
But times have changed. Since the invention of agriculture, and especially since industrialization, the environment has changed substantially and in many cases has come under our control, making some of these realities a lot less reliable. What happens when experiences necessary to our development are hard to find? Artificial light is much less bright than sunlight and seems to interfere with the normal matching of lens power to eye size by experience (see
Practical tip: Outdoor play improves vision
). Grocery stores are full of processed food, which lacks fiber, nutrients, and variety compared to our ancestral diet. Our brains have evolved to seek out sugar and fat because such foods were rare treats during our evolution, but now they are readily available. These dietary changes may contribute to the rise in obesity and some types of cancer.
These examples illustrate a fundamental conceptual problem with trying to separate the effects of genes from the effects of the environment: the two influences are inextricably linked (see
chapter 4
). Evolution has selected for genes that produced an adaptive outcome in our ancestral environment, but these genes may not interact as effectively with our current environment.
That doesn’t mean that there’s anything wrong with the modern world (we like our computers and antibiotics, thank you very much), nor that there’s anything wrong with our genes; it’s just that they don’t play nicely together in some cases. For instance, type 2 diabetes, which is linked to a variety of lifestyle risk factors, is also highly heritable. This may seem less confusing if you think of genes and environment as having a conversation about how growth should proceed. In this framework, particular genes and certain environmental conditions can easily interact to produce an unfavorable outcome that would not have resulted from variations in either the genes or the environmental conditions alone.
Visual experience also influences the development of face-recognition expertise starting in infancy. Six-month-olds are as good at distinguishing individual monkeys as individual people, but by nine months, babies become better at distinguishing people and lose the ability to discriminate among monkey faces. Starting between six and nine months of age, babies also find it slightly easier to distinguish faces within their own racial group than within other racial groups, probably because most babies have more visual experience with their own racial group than with others. This process, which is reminiscent of phoneme learning (see
chapter 6
), probably involves the sculpting of synaptic connections by experience to tune perception to the characteristics of the local environment.
Because our abilities build on one another, sensory deprivation during a sensitive period early in life can initiate a cascade of problems later on. This also means that aspects of vision that develop later are more sensitive to disruption than those that develop earlier. For example, babies cannot distinguish fine stripes from solid gray until their second birthday. Even so, babies who have cataracts from birth to six months of age never develop this ability, apparently because of residual damage to their primary visual cortex.
These findings suggest that parents should be particularly careful to protect their children from sensory deprivation early in life. A variety of problems, including cataracts, amblyopia, or strabismus, can prevent babies and toddlers from getting the experience that they need to help the visual system develop correctly. Strabismus occurs when the two eyes do not point in the same direction, which interferes with the development of binocular vision. Amblyopia occurs when one eye sees substantially less well than the other eye, though both are apparently healthy. It can be caused by strabismus or by near- or farsightedness that occurs
in only one eye. While strabismus or cataracts can be diagnosed by parents or doctors based on the appearance of the child’s eyes, amblyopia can only be identified by trained professionals.
Routine well-baby exams should catch most problems of this sort, but if your child is diagnosed with a sensory deficit (or you suspect that one exists), getting it fixed as soon as possible will minimize the possibility of lasting damage to your child’s brain. Amblyopia can be treated by several methods. Corrective glasses should be the first step, as this approach solves the problem in a quarter to a third of children and improves the amblyopia in others. The next step is to put a patch over the strong eye to force the weak eye to work harder. For all early visual difficulties, the most important point is to act quickly, before serious damage occurs.
Fortunately, problems in visual development are the exception. It’s amazing when you consider how complicated this process is, but in most cases, parents really can simply sit back and watch their children’s new abilities grow.
Chapter 11
CONNECT WITH YOUR BABY THROUGH HEARING AND TOUCH
AGES: THIRD TRIMESTER TO TWO YEARS
We have big brains. This is one of the things that distinguishes humans from other primates, and it has many consequences, some of them unexpected. One is that, because women’s hips are only so big, our babies have to be born before their brains have grown to full size.
As a result, the brains of infants are very immature. Newborn infants can’t roll over by themselves, and they can barely see, as we learned in the previous chapter. Some parts of their brains are relatively well developed at birth, though, including those devoted to the senses of hearing and touch, which provide the best ways to connect with your new baby.
Hearing begins when the ear receives a sound, a set of pressure waves that move through the air the way a splash ripples across a pond. The time between arriving waves (frequency) determines pitch, and their height determines sound intensity. The outer ear transmits these waves to the
cochlea
, which contains sound-sensing
hair cells
arranged along a long, coiled membrane (see
figure
). Sound pressure moves the fluid in the ear, which makes the membrane vibrate differently depending on the sound’s frequencies. This vibration moves a bundle of fine fibers that stick up from the top of the cell (hence the name hair cell), transforming the vibration into an electrical signal that can be understood by other neurons.
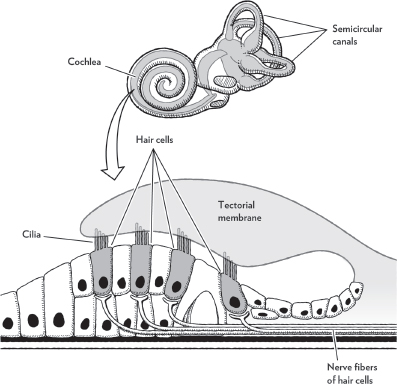
Hair cells at the base of the cochlear membrane sense the highest frequencies. As you move around the coil toward the other end, hair cells sense lower-frequency sounds. This organization forms a map of sound frequency, which is maintained in many of the brain areas that receive information that first passes through the cochlea. As in visual development, experience is important for fine-tuning connections in auditory brain regions, but the appropriate experience is easily available to any child who can hear.
A related group of organs in the inner ear, the
semicircular canals
(see figure), is responsible for sensing the head’s acceleration. This is called the
vestibular system
. These canals also contain hair cells arranged in a circle, where they are stimulated by calcium crystals—essentially little rocks that roll around inside the ear and settle on top of particular hair cells depending on which way is up. Imagine the beads inside a baby’s rattle; if you could feel the position of the beads, you’d be
able to work out which way it was pointing. This is what the brain is doing with information from the semicircular canals.
The vestibular system matures early, in the second trimester. It is vulnerable to many of the same factors that can disrupt hearing, including prenatal infections—particularly cytomegalovirus, a disease that accounts for 12 percent of congenital deafness—low birth weight, and bacterial meningitis in infancy. Disorders of the vestibular system can lead to developmental delay in motor function, as it is very difficult to learn to walk without reliable balance.
Babies can hear before they’re born, starting around the beginning of the third trimester. At this stage, they can hear only loud sounds at medium to low pitches—like a car horn or a truck rumble—which is convenient because those are the sounds that most easily reach the baby through the insulation of the mother’s belly. The mother’s voice also reaches the baby’s ears strongly because it is carried within her body. With time, the auditory system gradually becomes sensitive to quieter noises and higher pitches, a process that continues after birth.
Living near a loud highway could damage your child’s hearing as much as setting off firecrackers in her bedroom.
Auditory learning is already occurring during gestation. By the time they’re born, babies prefer their own mother’s voice to a stranger’s voice. Most newborns find the sounds that they’ve heard in utero to be soothing—anything from the theme song of Mom’s favorite soap opera to her heartbeat. They also prefer the sound of her language to a foreign language, probably because its cadence is more familiar to them.
At birth, babies are still less sensitive than adults to quiet or high-pitched sounds. A normal conversation sounds to a baby about as loud as a whisper sounds to you. By six months, frequency sensitivity is fully mature, allowing babies to hear high-pitched sounds. However, at this age loudness thresholds are only halfway to adult levels. Children’s ability to solve the
cocktail party problem
(discriminating a voice from background noise or from competing voices), a challenge that calls upon all of this information, continues to improve until age ten.
At all ages, children hear high frequencies better than most adults, whose
hearing has been damaged by too many loud sounds (see
Practical tip: Protect your child from noise, starting before birth
). Some teenagers take advantage of this situation by using high-pitched “mosquito ringtones” to prevent teachers and parents from hearing the ringing of cell phones in situations when they’re forbidden. Adults have turned the tables by using loud high-pitched sounds to prevent young people from loitering outside businesses or in parks (though we do not support this approach because it may harm the hearing of infants and toddlers whose parents are unaware of the noise).
Given the importance of hearing in a baby’s life, it is crucial to diagnose deafness in young children as early as possible. Nearly all babies are tested in the hospital at birth, but among those who are not, the average age of diagnosis is fourteen months, by which time auditory and language development are already delayed. Hearing loss can also develop in older babies due to infections or genetic problems with development. Parents should get their babies’ hearing tested if they don’t respond to sudden loud sounds or the voices of people who are out of their view.
Deafness resulting from damage to the cochlea can be treated with a cochlear implant, a device that transmits sound information directly to the auditory nerve. (If the deafness is due to damage in the brain rather than the ear, it usually cannot be corrected.) The signals sent by a cochlear implant are much less complex than the signals from a healthy cochlea, but the brain gradually learns to interpret the new signals correctly, especially if the implant is given in early childhood when the auditory system is best able to make adjustments. In general, cochlear implants can improve hearing at any age—but earlier is better.
The development of the sense of touch also depends on experience—in this case, provided by adult caretakers. Luckily, most people love to snuggle babies, so a lack of stimulation in this area is rare. Touch is critical for parent-infant bonding, which has an important influence on the baby’s emotional and cognitive development. Early touch also influences adult stress responsiveness in many mammals, including people (see
chapter 26
).
The neural pathways that carry information from the skin develop early in gestation, before any other senses. Your baby’s skin contains many different receptor types—specialized nerve endings that sense touch, vibration, pressure, skin tension, pain, or temperature (see figure opposite)—which are all in place by the end of the first trimester. Another set of receptors in muscles and joints provides information about body positioning and muscle tension. In all cases, touch is translated into the spikes we’ve been telling you about, and sent along axons into the spinal cord or brainstem.
